

Are you puzzled about MTHFR? Methylenetetrahydrofolate reductase (MTHFR) is an important enzyme for activating folate, and medical conditions can be linked to MTHFR genetic variants, decreased MTHFR enzyme activity, and/or reduced levels of methylfolate.
To understand why MTHFR enzyme function differs so radically among individuals, it is crucial to recognize why there are six common MTHFR enzyme phenotypes (or traits that can be observed). This understanding comes by recognizing three key insights.
But before you dive into this highly scientific explanation of MTHFR, be sure to brush up on the basics in this article covering what MTHFR is and how it can impact your health, or get a refresher in this article about how MTHFR functions in your body.
Three Key Insights That Explain Six MTHFR Enzyme Phenotypes
Insight 1: There exist both a MAJOR and a MINOR genetic variant that can impair the function of the MTHFR enzyme. The MAJOR genetic variant is at the 677 position, and the MINOR genetic variant is at the 1298 position of the MTHFR gene.
Insight 2: Each individual has TWO different versions (“copies”) of the MTHFR enzyme in their cells—a maternal version originating from the mother’s DNA, and a paternal version from the father’s DNA. Both enzyme versions exist in approximately equal amounts.
Insight 3: Both the maternal and paternal versions of the MTHFR enzyme can have either the MAJOR, MINOR, or NEITHER genetic variant (they are essentially mutually exclusive). Throughout the body, the maternal version of the enzyme has the major variant (at the 677 position) in about 35% of individuals, OR the minor variant (at the 1298 position) in about 30% of individuals, but almost NEVER BOTH genetic variants in the maternal copy of the enzyme. This situation is equally true in the paternal copy of the enzyme. This means both the maternal and paternal version of the enzyme each have about a 60-65% chance of having a genetic variant at either the 677 OR the 1298 site. The chance of the maternal version of the MTHFR enzyme being “optimal or normal” is about 35-40%, and this is equally true for the paternal version of the enzyme.
Let’s consider the implications of the three key insights above. What’s the chance that BOTH the maternal AND paternal versions of the MTHFR enzyme are “optimal or normal”? Simply multiply 35-40% chance (maternal enzyme) times 35-40% chance (paternal enzyme) to understand why only about 12-16% of individuals have two optimally functional copies of the MTHFR enzyme!
Another implication from the three key insights, is that there must be SIX common scenarios for MTHFR enzyme status within the population. This means six common “MTHFR enzyme phenotypes” as follows:
- Both (maternal and paternal) MTHFR copies normal (“homozygous normal”)
- One copy normal and the other copy with the minor variant (“heterozygous minor”)
- One copy normal and the other copy with the major variant (“heterozygous major”)
- One copy with the minor variant and the other copy with the minor variant (“homozygous minor”)
- One copy with the minor variant and the other copy with the major variant (“compound heterozygous”)
- Both copies with the major variant (“homozygous major”).
MTHFR Functional Activity
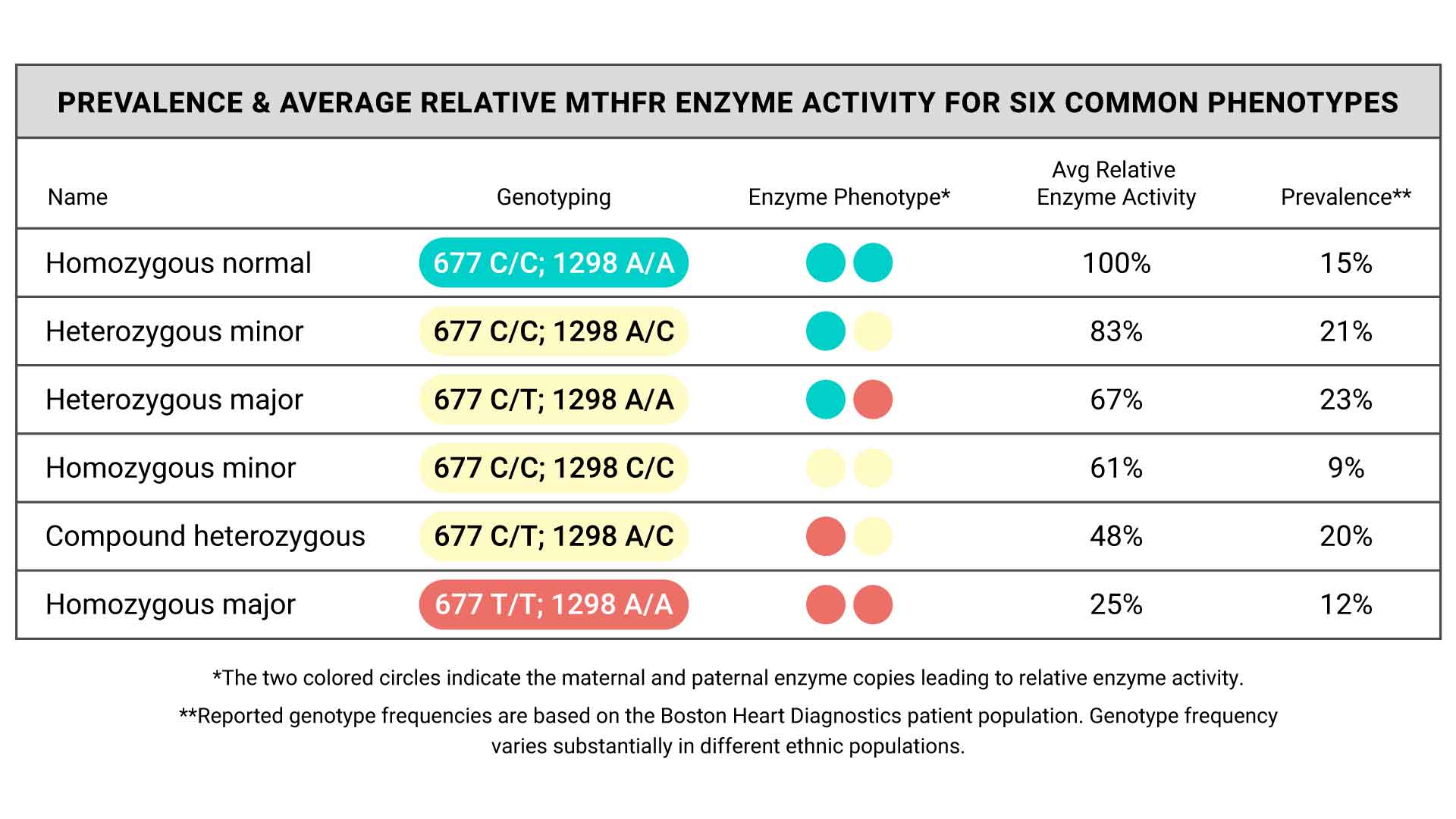
The table below summarizes the six common MTHFR phenotypes along with their total measured relative enzyme activity, and prevalence (within the Boston Heart Diagnostics patient population) of the corresponding genotype.
- Homozygous normal
- Heterozygous minor
- Heterozygous major
- Homozygous minor
- Compound heterozygous
- Homozygous major
MTHFR Enzyme Impairment is Common
The table above demonstrates that within a large population, partially impaired “suboptimal” MTHFR enzyme activity is commonplace. The relative degree of total MTHFR enzyme activity, which reflects the combined contribution from the maternal and paternal enzyme versions, is best when there is a normal copy from one or both parents. However, when both the maternal and the paternal copies have a minor or major genetic variant, then the combined enzyme activity is increasingly impaired, potentially reaching the threshold where physiological limitations in MTHFR enzyme function are more likely to have clinically meaningful and damaging impacts.
It is important to note that it is much more practical to characterize the MTHFR phenotype according to your DNA (MTHFR genotype), rather than your actual MTHFR enzyme activity (which is only a research tool rather than commercially available). There is wide variation around the average for each relative enzyme activity listed above. For example, not everyone with the “heterozygous major” phenotype has exactly 67% of the optimal enzyme functional activity, but the best data we have suggests that is the average. An individual’s MTHFR enzyme activity is largely determined by genetics, but also by other factors – for example, the availability or concentration of folate in cells, which depends largely on dietary and/or supplement intake.
MTHFR genetic variants are not “abnormal mutations”, and suboptimal MTHFR enzyme activity is not a “medical condition”. However, there are many medical conditions or health problems statistically associated with MTHFR status, and many clinicians are interested in using dietary/lifestyle strategies or supplements such as methylfolate or folic acid to potentially prevent associated medical conditions, especially in individuals at the greatest risk of impaired enzyme activity.
More research is needed in this area, but the clinical rationale for unmasking and potentially preventing conditions related to abnormal folate metabolism is based on a large body of existing scientific research.
Do I need treatment for an MTHFR variant?
So when does someone need treatment? Unfortunately there are limited data, and the decision requires clinical judgment based on clinical factors. Some healthcare providers may feel comfortable discussing methylfolate supplements in people with minor or major genetic variants in both enzyme copies (around 40% of the population), while others may reserve this approach solely for those with the major variant in both enzyme copies (around 12% of the population).
It makes good clinical sense to enthusiastically recommend good lifestyle habits for all, and consider supplements for certain individuals based on the combination of their MTHFR status, specific clinical factors that may compound the risk of associated preventable conditions, and emerging data related to treatment efficacy.
So, which MTHFR enzyme phenotype are you? Find out with an at-home MTHFR test, available from empowerDX!
Written by Dr. Michael Dansinger, MD, MS

{kind=link}